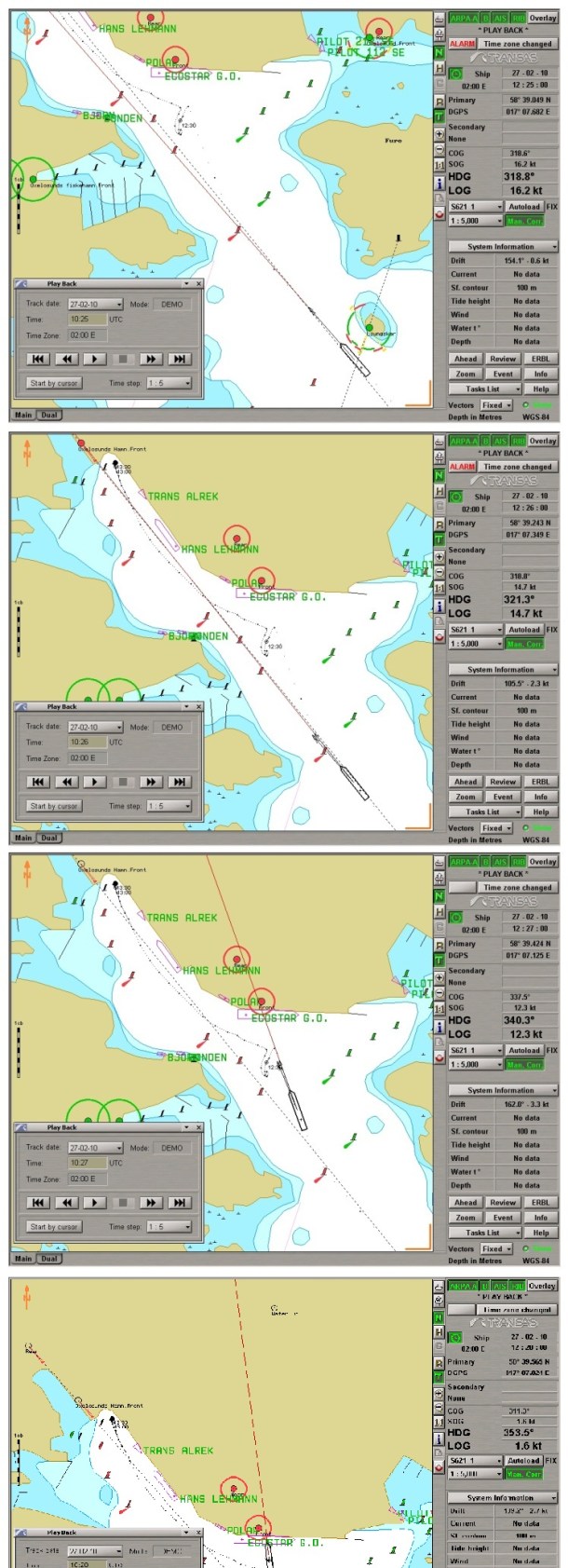
On 27 February 2010 the Finnish flagged vessel Global Carrier was on a routine voyage from Turku, Finland bound for Oxelösund, Sweden with a cargo of semitrailers and trucks. There was dense fog in the archipelago but pilot assistance was not considered because the Master was licensed to carry out piloting. The Master had previous experience of this fairway in similar visibility conditions. During a Global Carrier’s maneuver the vessel collided with the moored MV Ecostar G.O.

Global Carrier approached the archipelago with a speed of 16.2 knots and navigation was carried out by the OOW, the 1st Officer and the Master was on the bridge. Two radars were in operation, one in 0.75 NM range and the other in 1.5 NM range. The electronic chart display was also in use.
When passing Ljungskär the speed was still 16.2 knots and the distance to harbour was 0.6 miles. At this stage the Master was in charge of navigation. The speed was reduced to 12.8 knots after passing Ljungskär. There was no communication concerning the manoeuvres between the team members on the bridge. The speed should normally have been 6 knots when passing Ljungskär.
Chief Officer released the first Officer about ten minutes prior the approach to harbour. The Master did order the Chief Officer for look out as there was no dedicated watchman for lookout. By this order the Chief Officer lost his situational awareness.
Global Carrier collided with the alongside moored MV Ecostar G.O in Oxelösund port with the speed of 7.2 knots.

Global Carrier’s damages in the bow.

Top – The hole in Ecostar G.O.
Middle – The penetration effects in the cargo hold.
Bottom – An inside view from the wing tank of the Ecostar G.O.
According to SIA’s conclusions, the root cause for the accident can be considered to be
- The poorly implemented SMS routines onboard. The SMS for GLOBAL CARRIER was comprehensive but safety barriers that would have prevented this accident failed. Because all of the safety barriers failure it ended up in loss of situational awareness for the Officers on the Bridge. Due to loss of the situational awareness the safe speed was forgotten.
- The Master and the Chief Officer navigated in dense fog without outside references which made them dependent on the navigational equipment. There was no chance to react on the high speed spontaneously by watching passing objects. Since there were no reactions on the speed they proceeded with full ahead deep in to the harbour.
- The Master expected some ice in the Oxelösund archipelago and therefore the speed was not reduced in the first place when entering the archipelago.
- Since there was no speed limit in the fairway or in the voyage plan, the speed judgment was left for the Master alone. Even when there is no speed limit in a fairway the safe speed must always be considered.
- There was no communication between the Master and the chief officer on the bridge. The lack of communication is an indication of poorly implemented bridge resource management onboard.
There have been several accidents in recent years which have had rather similar factors as this accident such as lack of bridge resource management and insufficient voyage plan and/or execution and monitoring of the same. These factors have crucial significance especially when navigating in restricted waters such as archipelago. Applicable codes, guidelines and standards recommended by the IMO, administrations, classification societies and maritime industry organizations have been recognized and taken into account more widely in the tanker sector than in the dry cargo sector. These IMO, ICS, OCIMF and other guidelines have been available over a decade and are widely proven to increase safety in case properly implemented. The proper description and implementation of the before mentioned guidelines is not lonely enough as the compliance of the same should also be properly monitored by the Master and the company. In addition to the internal audits, one of today’s monitoring methods could be to collect recordings from the VDR to monitor the bridge resource management.
Source: Finland the Safety Investigation Authority













Leave a Comment