This investigation report refers to an explosion and a consequent fire in the forecastle of the 2159gt Isle of Man registered tanker Border Heather on 31 October 2004. As a result significant damage was caused to the vessel’s structure and systems but fortunately no-one was injured and there was no pollution.

Accident timeline
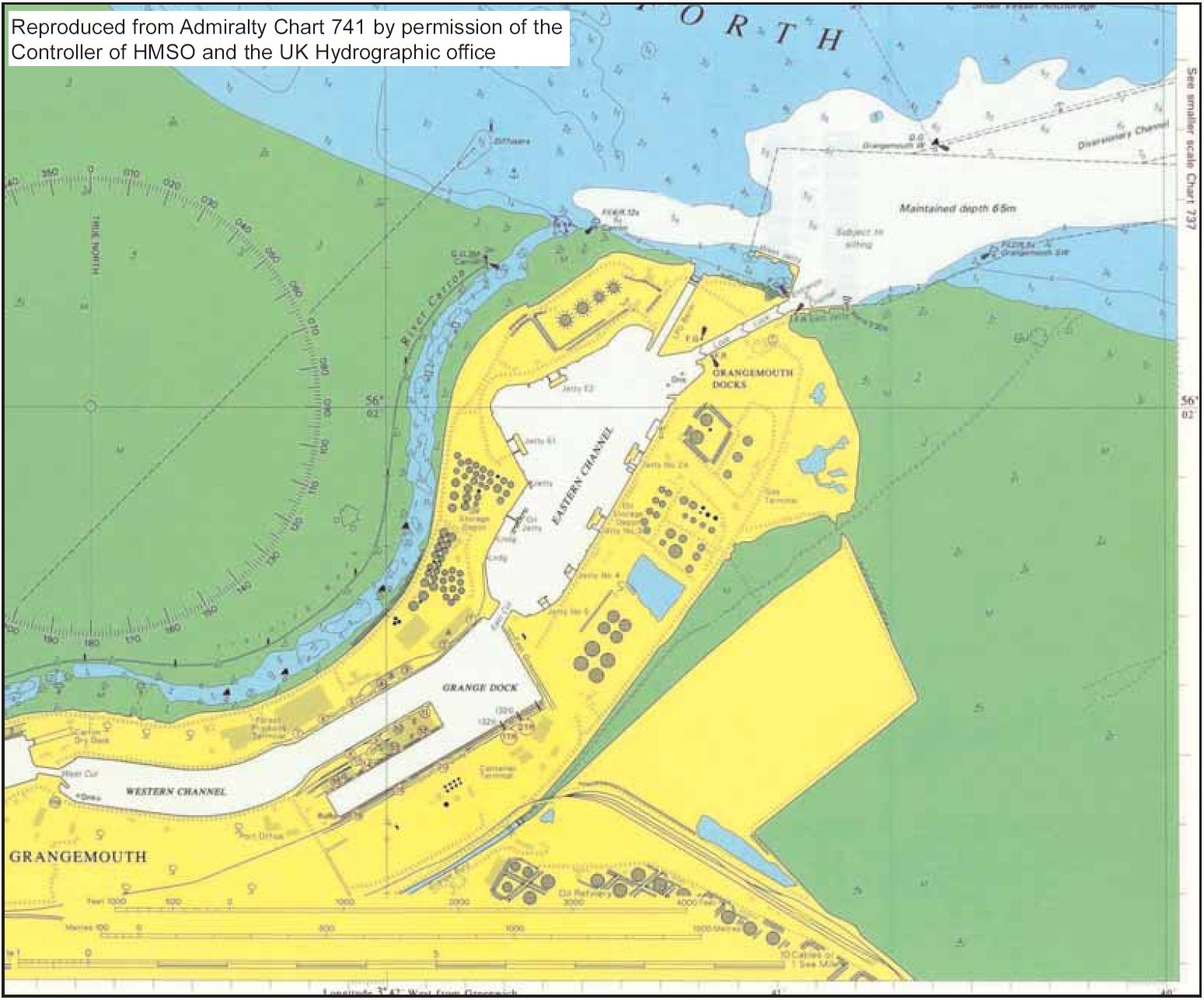
30 September 2004 – Following delivery to her charterers, BP Shipping, Border Heather arrived in Grangemouth. She loaded her first cargo of refined products in Grangemouth Docks (see figure below).
2 October 2004 – Border Heather left for the Orkney Islands . The cargo mentioned above and two further cargoes were delivered to ports in the Scottish Islands and Highlands. Each was loaded at Grangemouth. On each occasion the vessel’s gas freeing system was used to prepare the cargo tanks for loading.
27 October 2004 – Due to problems with the vessel’s fresh water cooling system she entered Grangemouth dry dock. This decision was made in order to repair to the fresh water heat exchangers in the sea chests. Prior to the dry-docking all cargo tanks were gas freed, using the vessel’s gas freeing system.
30 October 2004, 2200 hours – The necessary repairs were completed and the dry dock flooded in order to have the vessel afloat. During this time in order to retrieve a piece of cargo sampling equipment from number four starboard cargo tank, the chief officer started one of the gas freeing fans. He ran the fan for 10 to 15 minutes to freshen the tank’s atmosphere in order to make a safe entry. In the event, he did not climb into the tank, but used a boathook arrangement to retrieve the sampler. He then stopped the gas freeing fan, but did not close the valve on the fan or the interconnecting valve to the cargo system; his intention was to do that the following day before loading cargo. By that stage, it was about 2400 and he went to bed.
30 October 2004, 0900 hours – The vessel left the dry dock and berthed, starboard side alongside, at jetty number 4 in Grangemouth Dock to load cargo. She was alongside at 1000 (see figure below). Ship and terminal staff completed a ship/shore safety checklist and agreed a loading plan.

30 October 2004, 1110 hours – Loading of ultra low sulphur petrol (ULSP) into number one centre tank began through number one manifold (foremost).
30 October 2004, 1120 hours – Loading ultra low sulphur diesel (ULSD) into tanks two centre, four port and starboard began through number three manifold (aft).
30 October 2004, approximately 1130 hours – The duty second officer went into the purge air compressor room to shut down the compressor. As he left the compressor room, on the port side of the forecastle, he smelled petrol vapour. While investigating this smell he looked into the gas freeing room, on the starboard side of the forecastle, and noticed liquid coming from the casing of the forward gas freeing fan. He also saw a puddle at the forward end of the room, which he identified as ULSP. He then walked aft, to the cargo control room, and reported his findings to the chief officer. The two men returned forward, where the chief officer confirmed the second officer’s report and, after they had both returned to the main deck, closed the cross connecting valves between the gas freeing and cargo systems. The two men returned to the gas freeing room. The rate at which liquid was coming from the fan casing had much reduced. The ventilation fan for the gas freeing room was started and the ventilation flaps for the space opened. The two men then returned to their cargo loading duties.
30 October 2004, 1155 hours – Loading of ULSP into number one tank was complete and the lines were blown through.
30 October 2004, 1220 hours – Loading of kerosene began into number three port and starboard tanks, initially using number two manifold (centre). A crossover valve downstream of the manifold valve was not fully opened, which resulted in a line pressure of 16 bar being recorded ashore and caused a leak in the vessel’s cargo system. As a result, cargo operations were stopped and it was decided to recommence loading the kerosene through number three manifold (aft). Ship’s staff began to clean up the kerosene spill. The forecastle was again visited by the duty second officer, together with the vessel’s other second officer. They noticed that the amount of liquid in the gas freeing room had significantly reduced. They also visited the middle level of the forecastle and closed the hatch to the bow thrust room. Apart from the door of the gas freeing room, all other doors in the forecastle were closed.
30 October 2004, 1220 hours – Loading of ULSD was complete. The duty second officer again visited the gas freeing room. He noticed only very small quantities of liquid coming from the fan casing. He placed a plastic drum underneath the fan to collect this and, after scooping some of the liquid into the drum, wiped the deck beneath the fan dry. At this stage he could see no liquid elsewhere on the deck of the fan room.
30 October 2004, 1350 hours – Loading of kerosene recommenced Shortly afterwards, the duty second officer again visited the fan room. He found about 50mm of liquid in the drum beneath the fan but the deck was dry, no liquid was coming from the fan and the smell had diminished.
30 October 2004, 1500 hours – Loading kerosene was completed.
30 October 2004, between 1515 and 1615 hours – The remaining cargo was also loaded through number three manifold. This consisted of gas oil into tanks number five port and starboard.
30 October 2004, 1622 hours – Lines were blown through, and all cargo operations were finished. Shortly before loading was finished, the duty second officer again visited the forecastle. This time he went down to the middle level. Here he found a puddle of ULSP on the port side of the deck. He reported this to the chief officer. Throughout loading, the pressure recorded was between 1.9 and 2.1 bar (gauge) for all grades, except for the brief period shortly after loading kerosene began through number two manifold, when 16 bar was recorded.
30 October 2004, 1630 hours – On completion of cargo work, the loading hoses were disconnected.
30 October 2004, 1800 hours – Bridge equipment and steering gear were tested and the main engine was ready by 1800. At about this time the crew attempted to stow the gangway. The deck crane was malfunctioning and so the gangway was manhandled onto the deck for later stowage.
30 October 2004, 1820 hours – The crew were at stations. The master was on the bridge, with the chief officer; two able seamen (ABs) were on the forecastle; two second officers on the stern; the two engineers in the machinery control room and the cook in the galley. Two boatmen were on the jetty head to handle the mooring lines ashore. The main engine was clutched in. One of the ABs forward switched on power to the winches, using the switches just inside the forecastle access door. Engine control was passed to the bridge and power was switched onto the bow thruster at about 1820. Fore and aft lines were singled up.
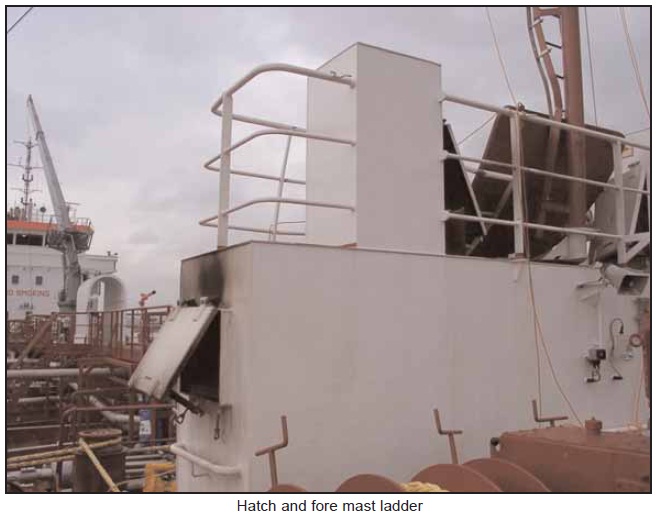
30 October 2004, 1823 hours – The master noticed that the bow thruster’s setting was not at zero. He gave the control a small nudge to correct this. Coincidentally with this adjustment there was an explosion within the forecastle head, throwing flame and burning material through the hatches, door and vents in the forecastle deckhouse.
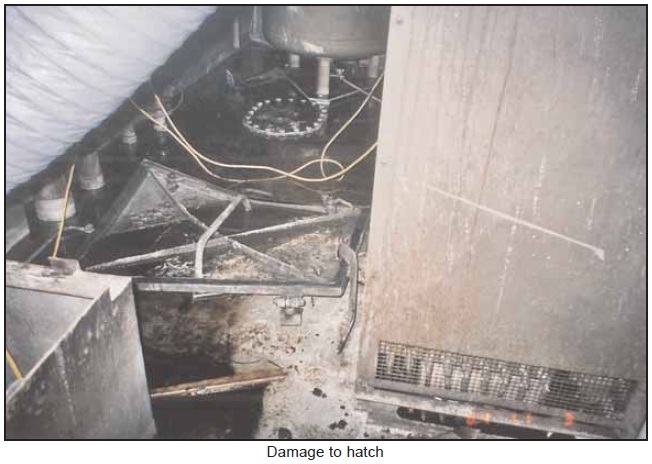
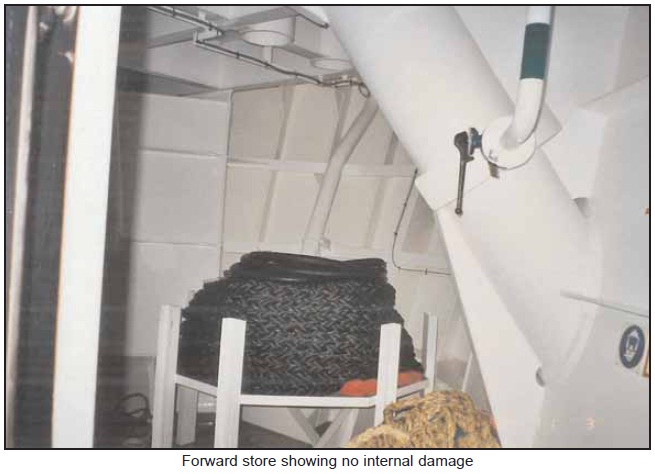
Photos below: As shown below all damage was confined to the forecastle structure and the systems and equipment contained therein.






One of the ABs on the forecastle head found himself hanging over the bulwark. He, and the second AB forward, decided they should clear the area and moved aft. The two boatmen on the jetty head turned away from the vessel and ran clear of the jetty area.
The vessel’s fire alarm was sounding and the fire display panel on the bridge indicated a ‘manual call’ in the forecastle. The master halted all mooring operations and tried to contact the ABs forward. He then radioed Port Control to report the accident, requesting fire-fighting assistance, and rang finished with engines. He also arranged for the chief officer to go forward, and telephoned the engine room to request electrical power to be shut off the forecastle and to tell the engineers of the explosion.
30 October 2004, 1825 hours – A member of the terminal’s staff, at an adjacent jetty, had heard the explosion and seen the resultant smoke. He activated the terminal’s shutdown procedure, which stopped cargo operations at jetty two, the only jetty working cargo. A colleague in the refrigerated liquid petroleum gas (RLPG) control room telephoned BP’s fire and security control room using the dedicated on-site three digit emergency number. He reported that an accident had occurred at jetty 4 about “two minutes ago”, he was able to see smoke from Border Heather and had heard a loud “bang”. After leaving the bridge, the chief officer collected overalls and other equipment from his cabin and went forward. The two second officers also made their way forward from the stern, as did the two ABs, the second engineer and the cook. The telephone call from the RLPG control room, to BP’s fire and security control room, automatically sounded a dedicated call tone throughout the fire/security complex. When this was heard by a first-aider in the adjacent medical centre, he moved to the fire and security control room to act as assistant to the controller, in accordance with standard emergency procedure.
30 October 2004, 1826 hours – After the explosion, the vessel’s forward foam monitor was activated by the crew. The master started the monitor’s pump at the bridge console. The running light on the console did not illuminate and the master pressed the start button again. This second depression caused the pump to trip, and the flow of water to the monitor stopped after only a few seconds. The master again attempted to start this pump, but it failed again and the crew abandoned their efforts to use the monitor. The master started the fire pump from the bridge console and two fire hoses were then rolled out and connected to the fire main. These were then used to cool the aft bulkhead and deck of the forecastle. One was also directed through the hatch in the top of the forecastle’s deckhouse. Smoke continued to issue from the hatch, door and vents of the forecastle deckhouse.
Having received an outline of the accident from the RLPG control room, the controller in the fire and security control room called out BP’s on-site fire teams and alerted on-site mobile security units at 1826. The controller’s assistant, without being instructed, activated the fire alarm that sounds only in the on-site fire station. The fire team members were then also called on their personal radios, which is in accordance with standard emergency procedure. However, the fire alarm did not sound in the on-site fire station.
30 October 2004, 1833 hours – Members of BP’s own fire service arrived on jetty 4.
30 October 2004, 1834 hours – Having confirmed details with BP’s on-scene fire officer, the fire and security controller called the Central Scotland Fire Brigade (CSFB). BP’s fire team was initially unable to board the vessel as no gangway was rigged. Three of the vessel’s crew manhandled the gangway into position, because of the problems with the deck crane.
30 October 2004, 1842 hours – The first firefighters, equipped with breathing apparatus (BA), boarded the vessel. Boundary cooling of the forecastle continued. Ship’s staff passed a Fire Plan to the fire team and assisted by supplying details of the forecastle arrangements.
30 October 2004, 1844 hours – Contact with the fire and security controller was made, using a private mobile telephone, by the fifth attending CSFB unit en-route to the accident. Thinking this was the first CSFB unit to attend, the controller requested that it approached jetty 4 by the south entrance, where a mobile patrol would be waiting and where they should hold. Mobile security staff were sent to the south entrance to the jetty area to open the gate and brief the CSFB. The gate was opened but the CSFB vehicles did not stop, they were driven straight into the jetty area.
30 October 2004, 1845 hours – The first units from CSFB arrived at the jetty area. These were two appliances and one platform. Four firefighters were wearing breathing apparatus on arrival.
30 October 2004, between between 1848 and 1908 hours – Four more CSFB units arrived.
Firefighters equipped with BA entered the forecastle. On reaching the bottom of the first stairway, at main deck level, they identified the seat of the fire as being in the gas freeing room. Visibility was very poor because of smoke.
Very little flame could be seen in the gas freeing room, but heat levels were high and visibility very poor. Using a fire hose set to jet and spray, the fire was tackled by firefighters from the doorway to the space. The firefighters suffered from the high levels of heat generated.
The bow of the vessel began to slowly swing away from the head of the jetty. Initially this movement was not noticed.
30 October 2004, 1908 hours – The fire in the gas freeing room was completely extinguished by the teams of firefighters, using fire hoses only. Inspection of the other forward spaces found no other fires, and the fire was declared out at 1908. Ambulance paramedics attended the vessel and assisted some of the crew who were showing ill effects from their recent experience.
Following these events, the spectacle plate between the discharge from the gas freeing fans and the cargo system was changed to the ‘blanked’ position (see figure below). Also, at about this time, the gap between the vessel’s bow and the jetty was noticed and extra lines were put out to secure the vessel.

30 October 2004, 2310 hours – Fire-fighting units left the scene.
Overnight, the atmosphere of the forward spaces was monitored for hydrocarbons. High levels were recorded until ventilation was begun and the spaces were pumped free of the water used during the fire-fighting.
Root causes
The following are the safety issues which were identified as a result of the investigation and may be considered as the root causes of the accident. They are not listed in any order of priority:
- There is little doubt that the chief officer was overloaded and fatigued as identified during the accident investigation (records of hours of rest where not available and there were statements that the chief officer took little sleep in general) by the evening before the accident, when he used the gas freeing system and decided to delay the proper shutting down of the system until the following morning. The forgetfulness of the chief officer, in not properly closing down the system the following morning, was just one consequence of this fatigue.
- The most likely cause of ignition appears to be either the electrical system associated with the bow thrusters, or that of the emergency fire pump; almost any electrical system within the space had the potential to have provided a source of ignition. Which one, is not considered critical.
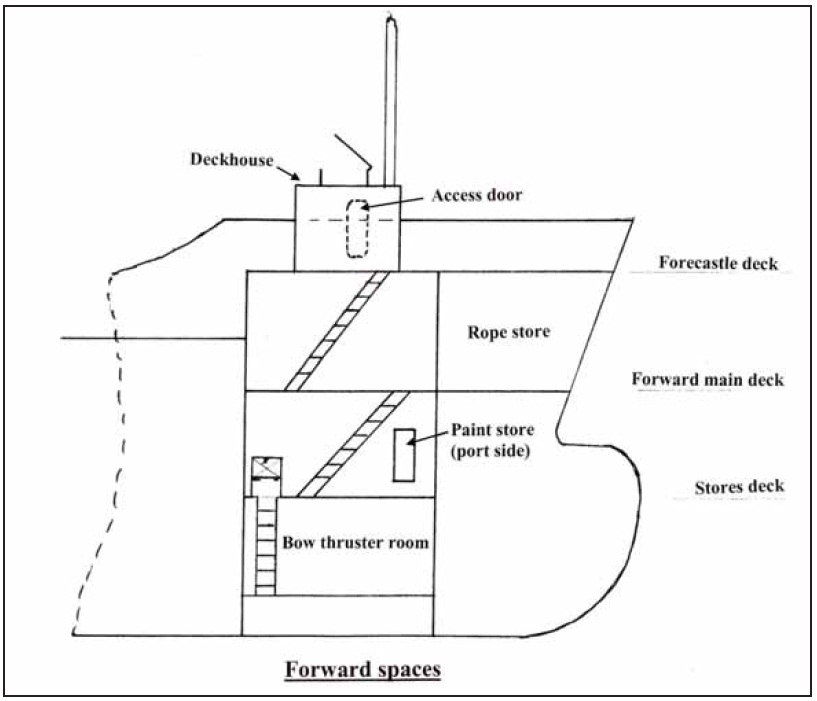
- ULSP cargo entered the gas freeing room of Border Heather, from the vessel’s cargo system, while the vessel was loading cargo. This was the result of isolation valves between the cargo and gas freeing systems not being closed and a non-return valve leaking. ULSP was then able to pass into the middle level and then, unnoticed, into the bow thrust space through the scuppers.
- The chief offer’s failure to tell the master of the leakage of ULSP into the gas freeing room was a misjudgement which, at least in part, was caused by a combination of his fatigue and his working relationship with the master; one that the chief officer found rather difficult as identified during the investigation report.
- The symptoms of the chief officer’s fatigue were again evident when ULSP was found to have drained to a lower level, and he decided that the forecastle could be cleaned up and made safe, without the need to report the situation to the master.
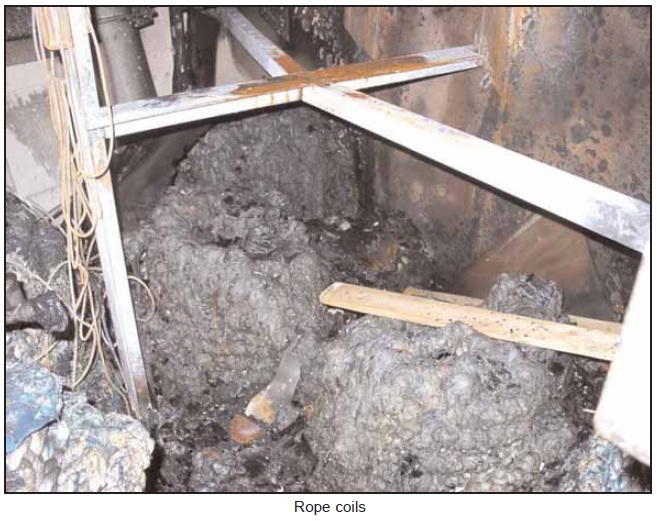
- The burning of the ropes contributed to the amount of heat generated, and certainly extended the duration of the accident, because the gas freeing room was effectively a vestibule for the forward rope store, although their temporary stowage in that space was not unreasonable.
- The non-return valve between the cargo and gas freeing systems failed to work as safety device to separate the two systems and prevent the type of accident that did happen.
- A spectacle blanking plate, intended to separate the cargo system from the gas freeing system, had not been put in the blanked position after the gas freeing system was last used.
- The guidance contained in ISGOTT would, if followed, have prevented cargo leakage into the gas freeing system and thus, also, prevented this accident.
- Ship’s staff looking for guidance on the use of the gas freeing system on Border Heather would have found only limited guidance in the SMS. They had to rely on information given by other staff, their own experience and initiative.
- There is little evidence that any of the deck officers on Border Heather attempted to find guidance in the SMS on the use of the gas freeing system. This was attributed, by some of them, to their high workload forcing them to take a ‘first aid’ approach to learning about the vessel.
- The company’s shore managers had some expectation that the delivery crew would begin the process of compiling operational data by undertaking risk assessments. Without guidance, the crew were unclear who should undertake this task and, consequently, no start was made on the process.
- The crew were reluctant to consult the vessel’s SMS for guidance, which was largely because the SMS remained in the boxes in which it had been shipped to the builder’s yard; it remained unpacked and almost inaccessible for a significant proportion of the vessel’s first few weeks in service.
- Inadequate emphasis was placed on the importance of commissioning the SMS, as it applied to Border Heather. Had the crew and the vessel’s managers given sufficient priority, at the time of delivery, to the need to carry out important initial processes, such as risk assessments, proper and safe operational procedures could have been drafted before the vessel loaded its first cargo. These could have been of great assistance to later crews.
- Better understanding of the company’s reporting system, and its objectives, might have prompted one or both of the deck officers to have reported the spill of ULSP to a person who had the authority to halt operations and so provided time to make the vessel safe.
- The crew on Border Heather at the time of this accident did not have the advantage of the extended period of familiarisation enjoyed by their predecessors. They were expected to overcome various problems and learn about a comparatively sophisticated vessel while operating her commercially.
- Following the explosion, one or two actions by the crew indicated a lack of familiarity with fire-fighting equipment, namely the incorrect donning of breathing apparatus and the problems experienced when attempting to start the pump of the foam monitor.
Lessons to be learned
- The non-return valve between the cargo and gas freeing systems was approved by LRS and fitted to perform the role of an ultimate safety device to separate the two systems and prevent the type of accident that did happen. Its failure so early in its working life suggests that consideration should be given to a change of design or specification for this item. While this valve should never have been seen as the sole isolator between the gas freeing and cargo systems, it was used in that way, albeit by default. However, it proved unable to serve the purpose for which it was fitted.
- In this case a spectacle plate and non-return valve had been fitted immediately aft of an isolation valve. However, the spectacle plate and isolating valve had been left in the open position and the non-return valve failed to function correctly. Special attention must always be given to such connections from nondangerous spaces to cargo tanks and cargo piping systems forming a dangerous zone. This applies to both plan approval surveyors and surveyors attending for the new building or any modification work.
- Where connections are required between non-dangerous spaces and dangerous zones, two non-return devices are to be fitted for isolation purposes. One of these devices is to provide positive separation by means of a spool piece or flexible hose which is to be removed when the line is not in use and blank flanges fitted. The other device is to be a non-return valve in accordance with an acceptable national or international standard appropriate for the design conditions of the piping system.
- HAZOP/HAZID process for critical systems should be made mandatory for all new build vessels, or for existing vessels being taken on, that will be managed. Critical systems will included Power to essential services, Propulsion, Steering, Cargo, Ballasting, Tank washing, Gas freeing.
- Use of a standard 5 day “hold” period between delivery of the ship and it sailing/entering commercial service. This period will allow comprehensive safety and security drills and testing of ship critical systems by ship’s staff, beyond those carried out and witnessed during builder’s trials. The 5 day “hold” period is in addition to the existing pre-delivery familiarization period that ship’s staff spend in the builder’s yard prior to delivery.
- Development of ship specific Operations Manuals is crucial. These manuals are in addition to the as built drawings and vendor’s manuals already placed on board. The Operations Manuals do not replace approved drawings or vendor’s manuals, and must always be used in conjunction with the approved drawings etc., but the Operations Manuals will provide the operator with a source of quick reference into the use of complete systems rather than individual components.
- Changes should be made in order to re-arrange and re-classify the gas freeing room as a hazardous area so as to be compatible with the deck cargo system.
Apart from the above and in connection with the incident, BP Shipping took a series of further preventive actions as indicated below in order to ensure that the accident will not occur again and to pass over lessons learned to any involved personnel onboad and ashore.
- Commencement of a 6 month period with an additional chief officer on each of the new vessels of the Border class, until the impact of the new vessels is better understood.
- Investigation of options to increase the number of berths on board, up to the limit of the LSA (12). This will ease existing restrictions to onboard training and familiarisation of staff.
- Evaluation of fire protective clothing (boiler suits) for use by ship’s staff. After trials on board, a final specification was to be developed for adoption across both domestic and international fleets.
- Launch of a staff Code of Conduct, which includes guidance to staff on confidentially reporting unsafe conditions and practices.
- BP Grangemouth has revised its Emergency Procedures, to include action plans for vessels to follow in the event of an emergency.
- BP Grangemouth has held a series of ‘toolbox’ talks with their technicians, highlighting the need to follow proper procedures during an emergency.
- Senior CSFB staff have given instructions and guidance to members of the fire teams attending this accident, on the safety precautions to be followed by all personnel when within the Grangemouth complex.
- BP Grangemouth and CSFB have agreed that selected officers from CSFB will attend BP site familiarisation courses and they will cascade the site safety requirements to potential attending firefighters. A quick reference card will also be produced by BP Grangemouth for CSFB staff.
Moreover, BP Shipping has modified the isolation and operation of the cargo/gas freeing system on Border Heather by:
- Replacing 10 bar butterfly isolating valve on deck with 20 bar working pressure double block and bleed valve.
- Replacing the non-return valve with one of a more suitable design.
- Replacing the simple spectacle plate blind with a swinging blind type, for easier use.
- Introducing a removable spool piece with adjacent signage requiring it to be out removed unless the gas freeing system is in use.
- Including an isolation verification step in the pre-cargo start up check-list.
- Introducing a permit system (Head Office approval required) for operating the gas freeing system (i.e. making the interconnection between the wet cargo system and the dry gas freeing system).
- Fitting a fixed gas detection system in the gas freeing fan room, with remote readout/alarm in the cargo control room.
- Including details of the new arrangements in the Cargo Operations Manual.
Source: MAIB













Leave a Comment