This accident investigation report refers to the fatal crush of a boatswain between the end stop for the crane’s trolley and the railings up on the walkway as the crane’s outriggers were swung in. None of the other persons who were up on the crane at the time of the accident observed the incident, but the ship’s management was notified as soon as it became clear that the boatswain had been crushed and first aid measures were implemented immediately. The ship’s management also called for medical personnel from ashore, who arrived quickly. Despite the steps taken, it was not possible to save the boatswain’s life.

At 1425, the chief mate instructed the crew on deck to start securing gantry crane no 1.The boatswain and the deck cadet, who were working in hold no 2 at the time, came up on deck and went up into the crane to start the work.
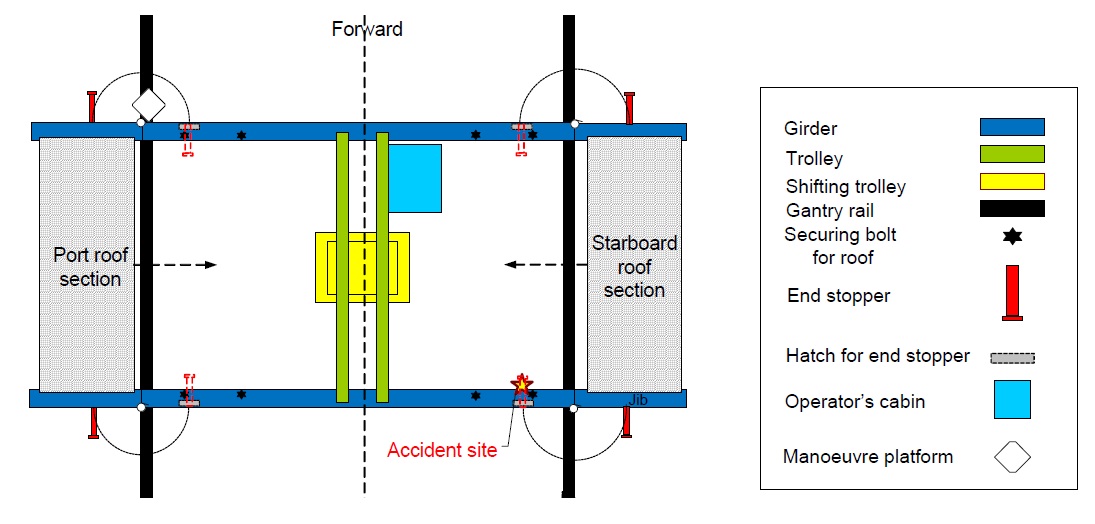
The boatswain was operating the trolley from the operator’s cabin located under the trolley at the forward edge. The trolley was attached to the sliding roof on the port side. The sliding roof was pulled towards the centre of the crane with the trolley. When the roof section was in right position, the cadet and boatswain secured it to the permanent roof structure with the four securing bolts (see simplified drawing of the gantry crane above). The electrician now came up and took over the operation of the trolley. The starboard sliding roof was attached to the trolley and run in towards the centre. The boatswain secured the roof section with the two securing bolts on the forward girder. The deck cadet secured the roof section with the two securing bolts on the aft girder.
The trolley was run to the centre position, whereupon the boatswain secured it at the forward end. He then went to the aft girder to show the deck cadet how to secure the aft end of the trolley. The electrician secured the shifting trolley at the centre of the trolley. When this part of the securing work had been completed, the boatswain, the electrician and the cadet stayed up on the crane. At 1430 the chief mate and the able seaman began to close the hatch of hold no 4. Gantry crane no 1 was used for this work. After the hatch was closed the chief mate went to the deck office and the seaman went to the manoeuvre platform to swing in the jibs.
As the view from the manoeuvre platform up to the forward and aft girders, where the rest of the securing work was to be carried out, is restricted, the seaman called up the electrician on his UHF radio and asked for the go-ahead to start the operation of swinging in the jibs. The boatswain, as well as the seaman and the electrician, had UHF radio communication. The electrician confirmed, by personal inspection, that both the cadet and the boatswain were in safe positions and gave the signal to go ahead. Having received the go-ahead signal, the seaman released the securing pistons for the jibs and started to swing in the jibs. The electric sensors confirmed that the sliding roof sections had been pulled in and secured, and the four jibs were set in motion.
At the time when the operation to swing in the jibs began, the electrician was on the trolley. The boatswain and the cadet were near the centre of the aft girder. Having given the go-ahead to start the operation to swing in the jibs, the electrician advised the boatswain that the hatches in the protective walls near the outer securing bolts, must be opened. The electrician moved forward on the forward girder and opened the hatches on both sides. He then left the crane superstructure and moved out onto the forward girder to observe the jibs during the closing process.
The boatswain told the cadet to open the hatch for the end stop at the port side of the aft girder. On his way towards the hatch the cadet saw that the boatswain was checking the work that he (the cadet) had done to secure the trolley. The cadet opened the port hatch and then checked that the sliding roof section was properly secured by the outer securing bolt, before moving inboard again, towards the centre of the girder. On his way in along the girder he saw the boatswain standing by the outer securing bolt at the aft end of the starboard sliding roof section (see simplified drawing of the gantry crane above). The cadet spoke to the boatswain, but received no answer. So he walked out towards the boatswain and saw that he had been struck by the end stop on the starboard aft jib. He shouted that the boatswain was trapped by the end stop. The seaman down on the manoeuvre platform heard the deck cadet cry out, realised that something was wrong and started to swing the jib back out.
The electrician also heard the deck cadet’s shout and went into the crane to find out what had happened. He saw that the boatswain was trapped by the end stop. As he ran towards the site of the accident, he used his UHF radio to report that there had been an accident and to summon help.
The electrician’s call on the UHF radio was received by the mate, who was on deck to oversee the transfer of three containers from hold no 8 to hold no 11, and by the chief mate and the captain, both of whom were in the office, in a meeting with a supercargo. They all ran to the site of the accident.
The time of the accident is estimated to be between 1445 and 1450. The ship’s mate, who was responsible for first aid and who received the electrician’s warning over the UHF radio, and the first aider from the facilities ashore, who was already on board, arrived at the site of the accident quickly and took over the treatment of the boatswain. At the request of the captain, the supercargo called for medical assistance from ashore. Medical personnel and the police came on board at approximately 1520. The ambulance arrived at 1530. Despite rapid treatment by the ship’s crew and the availability of external medical expertise, the boatswain’s life could not be saved. At 1617 the captain was informed by the supercargo that the boatswain had deceased.
Δθρινγ τηε ινωεστιγατιον ρεπορτ ιt has not been possible to ascertain why the boatswain was in the area of the outer securing bolt up until the time when he was hit by the end stop. After having opened the hatch for the end stop, he may have given his attention to checking the chain to be attached to the T-shaped securing bolt in the aft corner of the starboard sliding roof section. This is based on where the boatswain was hit and the position in which he was found, among other things. As brought forward from the company and the crew on board the boatswain was a highly responsible and conscientious seaman. In the light of the fact that the securing work in the aforementioned area had been carried out by an inexperienced cadet, it can be assumed that he was preoccupied with checking/attaching the aforementioned chain.
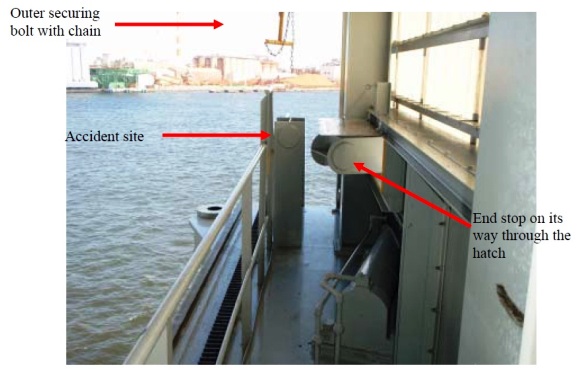
Once the accident occurred, it had the worst possible outcome. This is linked to the design and position of the end stops installed on the jibs to secure the trolley. These end stops move in through the crane’s forward and aft protective walls and pass the girders, and hence the walkway, at a height of approx. one metre just below the outer securing bolt for the sliding roof. Because of this, the Accident Investigation Board considers it necessary to look more closely at the actual design of the crane.
The investigation report conducted by AIBN concluded, among other, to the following safety recommendations:
- The fact that the end stops move through the crane’s protective walls without a sound, passing a walkway which may be occupied by personnel, is regarded as a safety problem. The AIBN recommended that the crane manufacturer should seek alternative solutions for new cranes.
- Personnel safety has been reduced by the development towards increasingly enclosed cranes and centralisation and transfer of the manoeuvre panels, combined with the choice of operational solutions whereby personnel are present up on the crane during the securing operation. The AIBN recommended that the shipping company, on the basis of a risk assessment of the crane securing operation, should review its procedures with particular focus on organisation, supervision and communication.
- The Regulations relating to shipboard loading and offloading appliances do not, already in the design phase, require risk assessments relating to the operation of the crane to be carried out. This may result in effective operational safety barriers not being incorporated into the crane design and hence personal safety will largely depend on the organisational aspects of crane operations. The AIBN recommended that the Norwegian Maritime Directorate review the above-mentioned regulations and consider whether they should include a functional safety requirement that would make it mandatory, already in the design phase, to conduct risk assessments relating to crane operation.
Source: AIBN













Leave a Comment