During the dismantling of scaffolding on Oseberg B 7 May 2009, a scaffolder was seriously injured as he fell 14 meters from the scaffolding and down on to the cellar deck. He was evacuated by rescue helicopter to Haukeland hospital in Bergen, and later died at the hospital.

Accident timeline
The description of the course of events is based on interviews of personnel on board and investigations at the accident site.
In order to carry out maintenance on a searchlight, a scaffolding was erected on Oseberg B on 24 April 2009. The maintenance work was completed a few days before the accident on 7 May 2009, and the scaffolding company (STS), through the foreman, had decided to dismantle the scaffold in question in order to access scaffolding material for another assignment.
The scaffold was a partly hanging scaffold, and the dismantling was considered to be a routine operation. The scaffolding in question was not defined as safety critical in terms of safety for the scaffolder. The scaffold had already been approved for use and marked with a green “tag”.
Dismantling was planned for the evening of 6 May 2009, but due to a rush assignment on Oseberg D, the work team was sent there to assemble a scaffold. The dismantling was as a result postponed to Thursday morning, 7 May 2009. A new work team was assigned the dismantling job the same morning.
The work permit for the job was valid for the period 1 May to 8 May 2009, but in order for the platform management to have overview of on-going work, all work permits had to be approved for each day. The work permit in question was approved on the morning of 7 May 2009 and was signed by the area technician and the executive the professional who was to perfom the work. These checklists mainly deal with risk in connection to the relationship between the scaffolding and the users/environment.
The assembly guidelines from the manufacturer were of a general character and were not normally used when planning assembly and dismantling. It is not common practice to draw up work instructions for assembly and dismantling of individual scaffolds.
The work team assigned to carry out the dismantling was composed of three persons,
- A: The person who died in the accident
- B: Person being trained
- C: Person who collects and signs the work permit
Before the work starts, A, B and C have a Tool box Meeting (TBM) and review the checklist for scaffolding work. During the talk it was not clarified who will lead the work team. The dismantling was regarded as a routine assignment, and risk factors in connection with the dismantling were not discussed.
While C leaves to have the work permit approved, A puts on the fall safety harness (Y-line) and B goes down to the cellar deck to cordon off the area under the scaffold. After cordoning off the area, B returns to the scaffold on the lower deck. There they wait for C to return with an approved WP, so they can start work. Due to an upcoming lifting operation, they are told to wait and B removes the cordons. When they are told after a short period of time to start the dismantling, B goes down to the cellar deck and cordons off the area again.
The photo below shows the remaining scaffolding parts after the accident. The scaffold was a partly hanging jack scaffold. The one end was on the deck (standard 8 and 9) and the other end (standard 3), with jack, was suspended by chain (1) from an H-beam on the deck above.
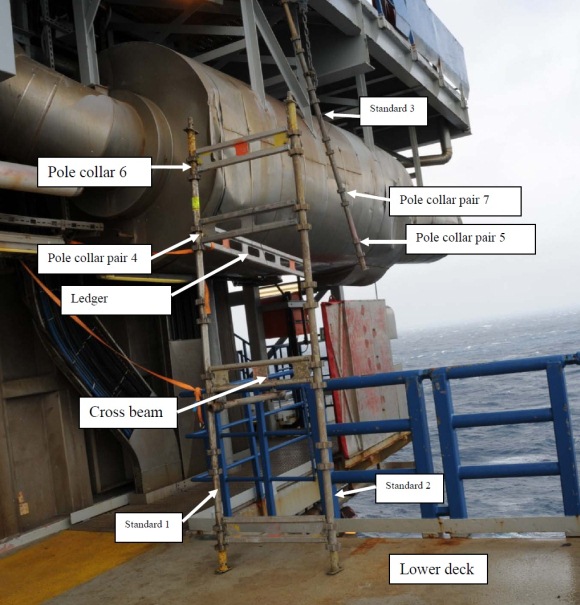
While B goes down to the cellar deck to put up new cordons, A and C start the dismantling. A stay cable/pipe attached between standard 3 and the rails to brace the scaffold, was removed first. Then they commenced dismantling from the top of the scaffold.
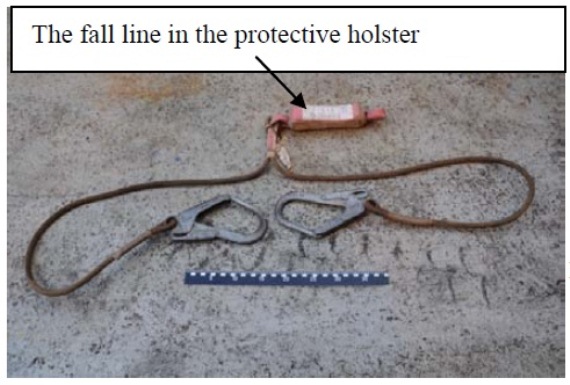
Photo showing the Y-line with hook 1 and hook 2
While B goes down to the cellar deck to put up new cordons, A and C start the dismantling. A stay cable/pipe attached between standard 3 and the rails to brace the scaffold, was removed first. Then they commenced dismantling from the top of the scaffold.
Before the accident, A walks out on the ledger fastened to the pole collar pairs 4 and 5. He holds on to the ledger which at the time was fastened to polar collar pairs 4 and 5, and had attached the one hook of the safety harness to ledger 6-7 (hook 1 in the Y-line, see photos). The other hook (hook 2) on the Y-line was attached to hook 1. He opens the latches which lock the ledgers 4-5 and 6-7 to the pole collars on standard 3 (see photo above). This was done so that they later could remove the ledgers while standing on the lower deck.
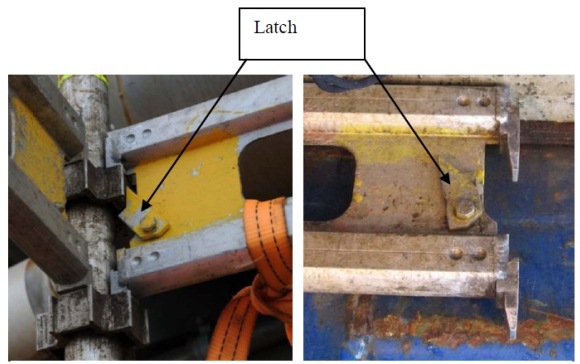
In a preassembled scaffold, the ledgers are attached to pole collars (fastening arrangement on the standard to which the ledger is attached) at the scaffold standards in each end and locked in place by latches. The latches prevent the ledgers being lifted out of the pole collars to which they are attached. The photo to the left shows the ledger attached to the pole collar pair and the latch in the locked position. The photo to the right shows the latch in the open position.
In order to find a new point to fasten the safety harness, A was about to unfasten hook 1 from ledger 6-7. B made him aware that he should not unfasten hook 1, but used hook 2 (which at the time was attached to hook 1) to secure the harness to a new point.
A is on his knees on ledger 4-5 and holding on to ledger 6-7. As he gets up to find a new fastening point for hook 2, ledger 6-7 is lifted out of the locks on pole collar 7. This results in the running, to which he is holding onto with his hands, turns sideways and he loses his footing on ledger 4-5. For a brief moment he hangs from ledger 6-7 which is now only attached to pole collar 6. Pole collar 6 cannot withstand the load and breaks, and consequently, A, together with ledger 6-7, falls 14 meters to the cellar deck. During the fall, ledger 4-5 is also lifted out of the locks on pole collar pair 5.
The accident occurs at around 0855 hours. Immediately following the accident, C runs to report the accident, while asking B to look after A on the cellar deck. C then triggers a fire alarm and dials the 112 emergency number. The notification was registered in the control room at 0855 hours.
When B arrives at the accident site, he sees that A is conscious. The next to arrive at the accident site, is the deck supervisor at about 0903 hours. A first aid team arrives shortly after, and provides first aid to A. The patient arrives at the hospital on the facility at 0920 hours. At 0945 hours he is evacuated by SAR helicopter to Haukeland University Hospital, where he later dies.
Root causes
- Insufficient risk assessment: The person in charge had not ensured a broad and sufficient assessment of the risk for the scaffold installers when assembling and dismantling.
- Insufficient planning: The dismantling of the scaffold was insufficiently planned.
- Insufficient competence: It had not been ensured that the personnel had the necessary competence to carry out the activity in a safe and secure manner.
- Insufficient clarification of leadership and roles: Responsibility and authority were not clearly defined at all times during planning and execution of the dismantling.
- Insufficient governing documents: Governing documents did not safeguard the regulatory requirements for safety for scaffolders.
- Insufficient maintenance of supervisory duty: StatoilHydro did not ensure that Aibel and STS had management systems which safeguard the safety of scaffolders.
- Lack of use of radio: The work team dismantling the scaffold did not have radios.
- Cordoning off area before dismantling the scaffold: The work team cordoned off the decks below in compliance with the applicable procedure.
Lessons learned
- A written work description for working on scaffolds should be prepared
- The correct use of fall arrest equipment must be ensured
- It is recommended that SJA is used for larger scaffolding systems and hanging scaffolds.
- New personnel must be followed up in a satisfactory manner.
- A practice where new personnel are integrated in the team before they are assigned independent tasks should be implemented.
- Gullfaks should ensure systematic controls to make sure personnel who arrive at the facility comply with time off requirements in accordance with the working hours regulations in the Norwegian Petroleum Directorate’s “Regulations on the protection of workers and working environment in the petroleum industry”, Section 19
- Self-monitoring should be improved.
- It is recommended that Statoil review its routines to uncover violations of working hours regulations.
Source: PSA Norway













Leave a Comment