This incident information refers to an accident that occurred onboard an offshore platform in the Gulf of Mexico during maintenance and repair operations to clean several production vessels, including a high-pressure separator, the floatation cell, the wet-oil tank, and two stacked low-pressure separators, upper and lower. A flash fire ignited within one of the vessel’s causing injuries to four crew members.

Accident Timeline
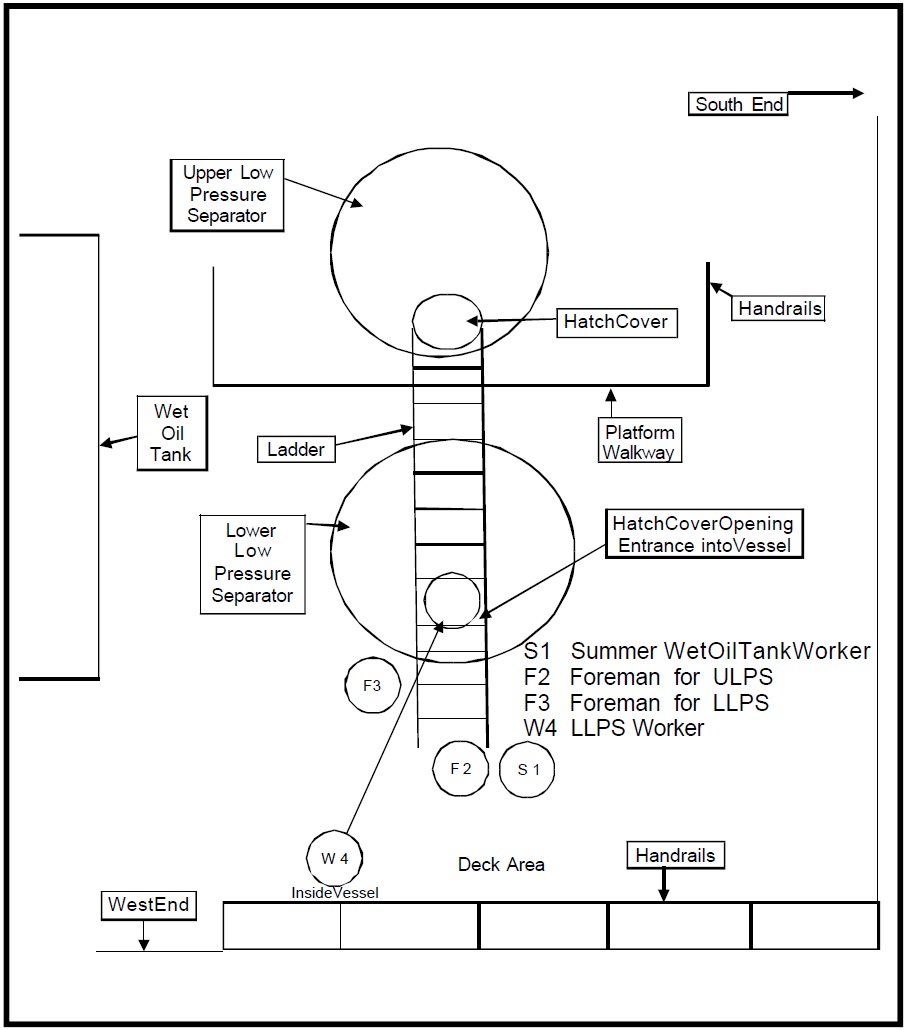
On the shifts described below, the Contractor crews were organized into three groups of three men, each supervised by a foreman reporting to the project manager. Contractor personnel on the nightshift included the project manager; three foremen, including the foreman for the upper low-pressure separator and his three crew members; the foreman for the lower low-pressure separator and his crew, which included the worker assigned for confined space entry; and the foreman for the wet oil tank and his crew. The wet-oil tank crew included one new temporary employee working for the summer. By Contractor policy, a new or inexperienced employee was assigned a mentor until he was deemed fully qualified. All foremen and crew members were trained with both formal schooling and experience. (figure below for diagram of platform vessel location.)
7 June 2002 – The Contractor rigging crew unloaded the equipment necessary for the cleaning operation onto the Platform.
11 June 2002 – After the “super safety session” conducted by the Operator for all contract crews involved in the turnaround, Contractor crews were transported to the living quarters on South
Timbalier Block 130 Platform.
12 June 2002 – Operations commenced on the Platform by transporting the day shift from South Timbalier Block 130 to the Platform. The Operator specified the work to continue on a 24-hour a day basis and, as such, the Contactor provided two full work shifts that included three foremen on each shift. The day shift attended a pre-work safety meeting conducted for all contractors by the Operator and additional meetings specific to the task at hand conducted by the project manager. They set up the equipment needed to begin the cleaning operations on the floatation cell, the wet oil tank, and the high-pressure separators. Isolation of the vessels to be cleaned was performed by double block and bleed and skilleting. The night crew relieved the day crew at 1800 hrs. After a safety operations meeting conducted by the Operator, and another meeting specific to the job at hand conducted by Contractor personnel, the shift work preparation continued by writing the Job Safety Analysis (JSA) for each individual task. The shift then continued operations begun by the day shift, including pumping out the floatation cell and transferring the fluid in the wet-oil tank to the dry-oil tank.
13 June 2002, 0600 hours – The crew change was initiated with the day crew relieving the night shift. They first attended the Operator-conducted safety meeting, followed by the project manager’s meeting that outlined the work scope for the shift. The crews then wrote JSA’s. Isolation of the wet-oil tank was completed and, after ventilation and gas testing, a confined space entry into the wet-oil tank was made to initiate removal of the debris. Gas detection testing of the floatation cell indicated the presence of an unacceptable level of hydrocarbons, which prevented initiation of confined space entry into that vessel. Therefore, ventilation and flushing continued until an acceptable gas test reading was obtained. After the crew change at 1800 hours and the completion of the usual safety meetings, scope discussion, and the writing of the JSA’s, cleaning of the wet-oil tank continued and cleaning of the floatation cell was initiated. Additionally, the high-pressure separator was isolated, ventilated, and tested for gas in preparation of cleaning operations. After removal of the fluids, entry into the high-pressure separator was initiated and the vessel was cleaned of all sand and debris, which were transferred to the cuttings boxes. Upon completion of the cleaning of the high-pressure separator, that vessel was prepared to be returned to service.
14 June 2002, 0600 hours – The day shift came on duty, conducted the Operator and Contractor safety meetings, job scope discussion, and the writing of the JSA’s. According to testimony, two engineering personnel from the Operator discussed the need to speed up the work to return to production as soon as possible. Instructions were given to the Contractor project manager to complete cleaning of the upper low-pressure separator and lower low-pressure separator by about 0800 hours on 15 June 2002 or forgo that particular operation. The stated reason for this request was to complete the work concurrently with completion of the other contractor’s activities so as to return the Platform to production as early as possible. Confined space entry work continued in the wet-oil tank and cleaning of the floatation cell was completed. The high-pressure separator hatches were secured.
14 June 2002, 1930 hours – The night shift completed the crew change. Operator personnel conducted a meeting with the supervisors for several different tasks including the Contractor’s operation. After the shift meeting, the Contractor foremen conducted their own JSA meetings. The crew went through the standard hazards and held a walk-through with the project manager and Operator’s production personnel, checking the position of the valves, whether they were blocked and bled, etc., including a discussion of the condition of the piping connected to the vessels. The inlet valve for the lower low-pressure separator was reported to be double blocked and bled. However, subsequent investigation could not determine the actual position and condition of the bleed valve.
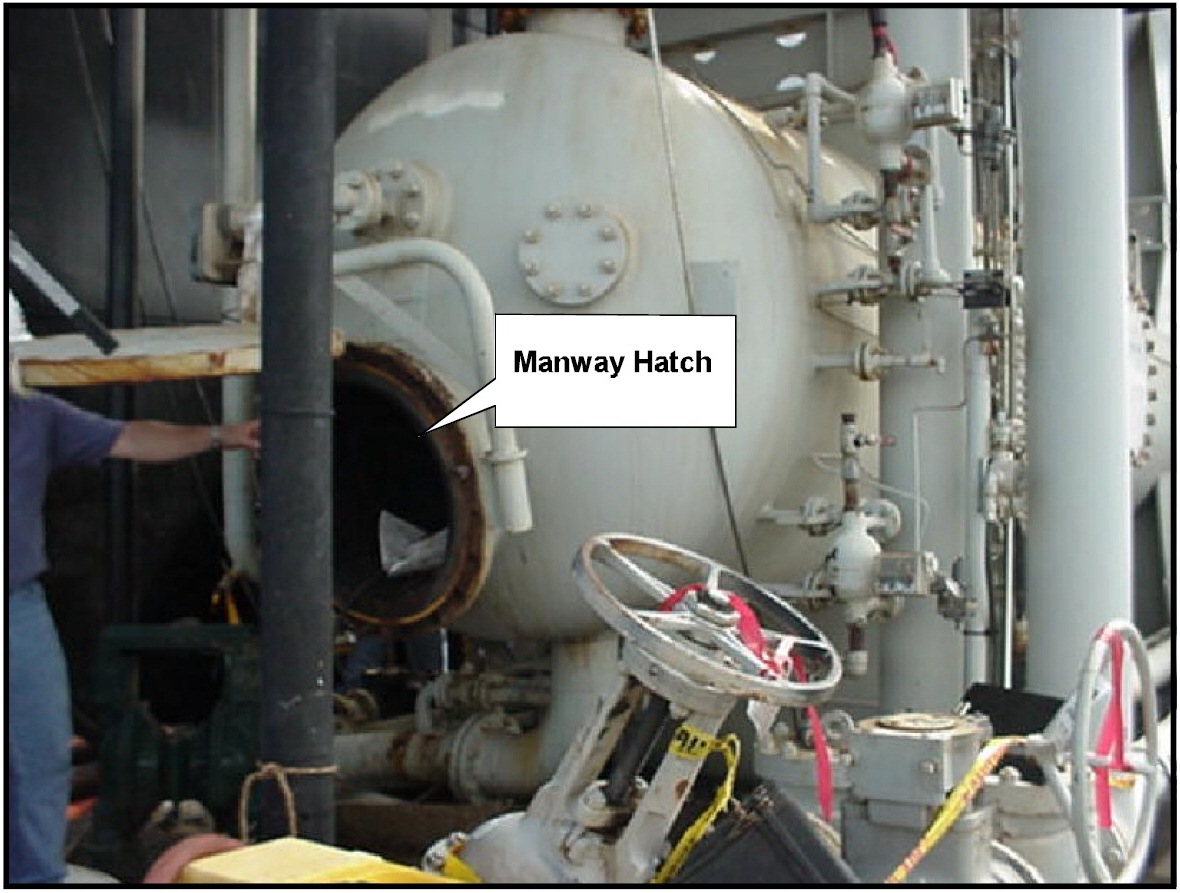
14 June 2002, 2000 hours – The lower low-pressure separator crew set up and began draining the vessel and opening the manway hatch. The foreman for the lower low-pressure separator then filled in and signed his entry permit slips, allowing personnel to initiate confined space entry.
14 June 2002, 2100 hours – The project manager reached the limit of continuous workhours under the work rules of the Contractor. These work rules required him to go off duty and rest. He reviewed the ongoing work being conducted on the three vessels and assigned the foreman for the wet-oil tank the additional responsibility of acting as overall contact point to coordinate the work on all of the vessels if any necessity should arise. According to testimony, in the event of an uncertainty as to procedure, he was instructed to wake the project manager for guidance.
14 June 2002, 2130 hrs – The lower low-pressure separator crew drained the fluid off the separator and removed that vessel’s manway hatch. The foreman for the lower low-pressure separator then took a measurement through the manway by using a gas detector, which returned a negative reading. (see figure below for schematic of positioning of upper low-pressure separator and lower low- pressure separator.) The foreman then reached into the vessel and checked the vessel’s contents nearest the hatch with the gas detector, which again returned a negative reading. It should be noted that breaking the plane of the hatch technically constituted a confined space entry, for which the foreman was not equipped properly. A crew member then suited up with protective clothing and made a confined space entry to begin washing the tank. The crewman used a suction hose to clean out the inlet side of the tank adjacent to the manway hatch, getting primarily water. Thereafter, he attempted to wash out the sand, eventually clogging up the pumpjust prior t o a break for the mid-shift meal. For this operation on the lower low-pressure separator, the crew did not follow published Contractor and Operator safety requirements that called for opening the second hatch accessing the vessel and ventilating for a period of time, and continuously ventilating during any entry. They also only tested for hydrocarbon presence near the hatch of the open manway and did not follow company policy when the plane of the hatch was broken by the supervisor checking with the gas detector. The upper low-pressure separator cleaning crew began preparing the separator for confined space entry by beginning the removal of the manway hatch bolts. Simultaneously, the crew cleaning the wet-oil tank was preparing to initiate a confined space entry.

14 June 2002, 2300 hours – The Contractor crews broke for midshift meal. According to testimony, during the break Operator personnel requested that the Contractor arrange for the retrieval of a sample of the sand and debris from the lower low-pressure separator. This request was passed to the foreman for that operation.
15 June 2002, 0030 hours – The crews resumed activities, with the wet-oil tank crew continuing to prepare for further confined space entry. The crew on the upper low-pressure separator continued to break the bolts, preparing to ventilate the tank and initiate cleaning operations. At the direction of the foreman for the lower low-pressure separator, a crew member prepared for a confined space entry to continue cleaning the vessel and to retrieve the previously requested sample. After testing the area of the manway hatch with a gas detector, the foreman again reached into the vessel through the hatch and tested for the presence of hydrocarbons, with negative results. It is unclear whether he used the gas detector in the upper part of the vessel.
The crew member carrying out the confined space entry was equipped with all required equipment, including suit, breathing air, boots, gloves etc. He had with him a plastic sample jar and an approved explosion-proof flashlight. He proceeded behind the weir, about two-thirds to three-quarters of the way to the back, and bent to take a sample. This area of the vessel had not yet been disturbed by washing, and the sand, scale, and debris were between one-inch to one-foot thick in the bottom of the tank, with a thin covering or film of oil and water.
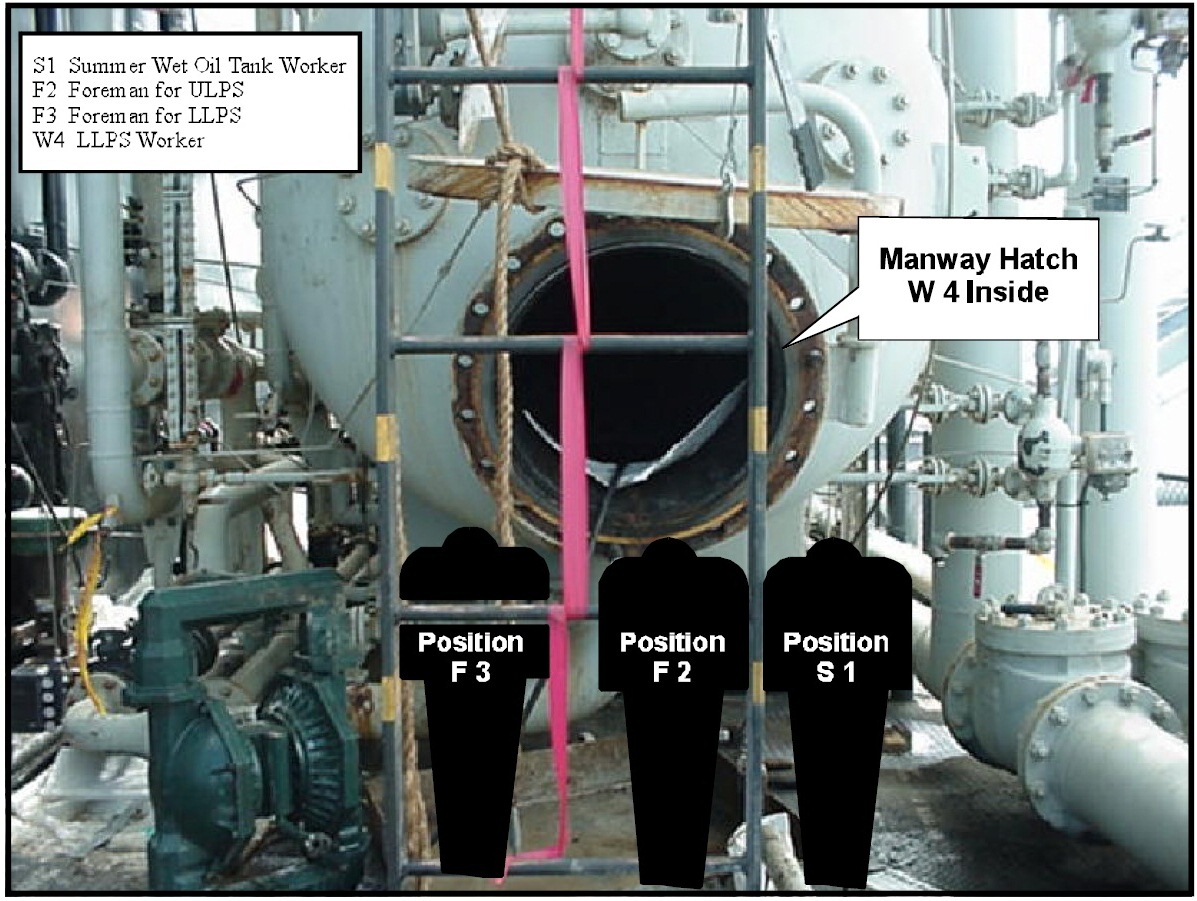
At this moment, the crew working on the upper low-pressure separator encountered difficulties in fully opening the manway hatch because of a frozen swing arm mechanism. The foreman for the upper low-pressure separator came down the ladder to speak with the foreman for the lower lowpressure separator about the problem, standing in front of the manway hatch of the lower lowpressure separator. The foreman for the lower low-pressure separator had watched the confined space entry progress of his crewman to retrieve the sample, until he could no longer see the crewman through the manway. He then stooped to adjust the nozzle of a soap sprayer that he had begun using to clean the outside of the vessel of some residual oil. Simultaneously, the summer worker assigned to the crew cleaning the wet-oil tank was passing the lower low-pressure separator, having been sent to retrieve additional protective gear. He stopped beside the foreman for the upper low-pressure separator and inquired what was being sprayed on the lower lowpressure separator and why. (see figures above and below for position of crew members as well as for a picture of stacked lower low-pressure separator and manway hatch, and position of crew.) The weather was hot and humid with occasional heat lightning observed in clouds on the horizon. On another platform connected by a bridge, a welding crew from another company was conducting welding operations.
15 June, 0045 hours – The crewman inside the lower low-pressure separator moved toward the back of the vessel, faced the right-hand wall, and bent down to fill his sample jar. A flash explosion, described as a fireball, suddenly proceeded across the upper part of the vessel and out of the manway hatch. Some accounts indicate the fireball was accompanied by a rushing or rumbling that reverberated in the pipes.
The fireball passed over the crouching crewman inside the separator, who felt the heat before hearing anything. He rapidly exited the vessel, diving over the weir and out the manway. In the Fprocess, he hurt his shoulder and received second-degree burns on his forearm, neck, and left ear. As the fireball exited the manway, the blast passed over the crouching foreman for the lower lowpressure separator, who was adjusting the soap nozzle. He heard a rumble, followed by a concussion and blast that knocked him down and left a ringing sensation in one ear and redness of the skin on one hand. The foreman stood up, turned, and saw one man down on the platform. Meanwhile, the exiting blast directly impacted the two employees observing the operation while standing in front of the manway hatch. The foreman for the upper low-pressure separator was propelled by the blast back against the guardrail fence. The fireball burned off most of his trousers and the impact of his body against the guardrail/cyclone fence, or flying debris, produced numerous bruises and a puncture on his right leg from an unknown source. Approximately 40 percent of his body had first- or second-degree burns, with about 15 percent of his body receiving second- degree burns, primarily near his midriff.
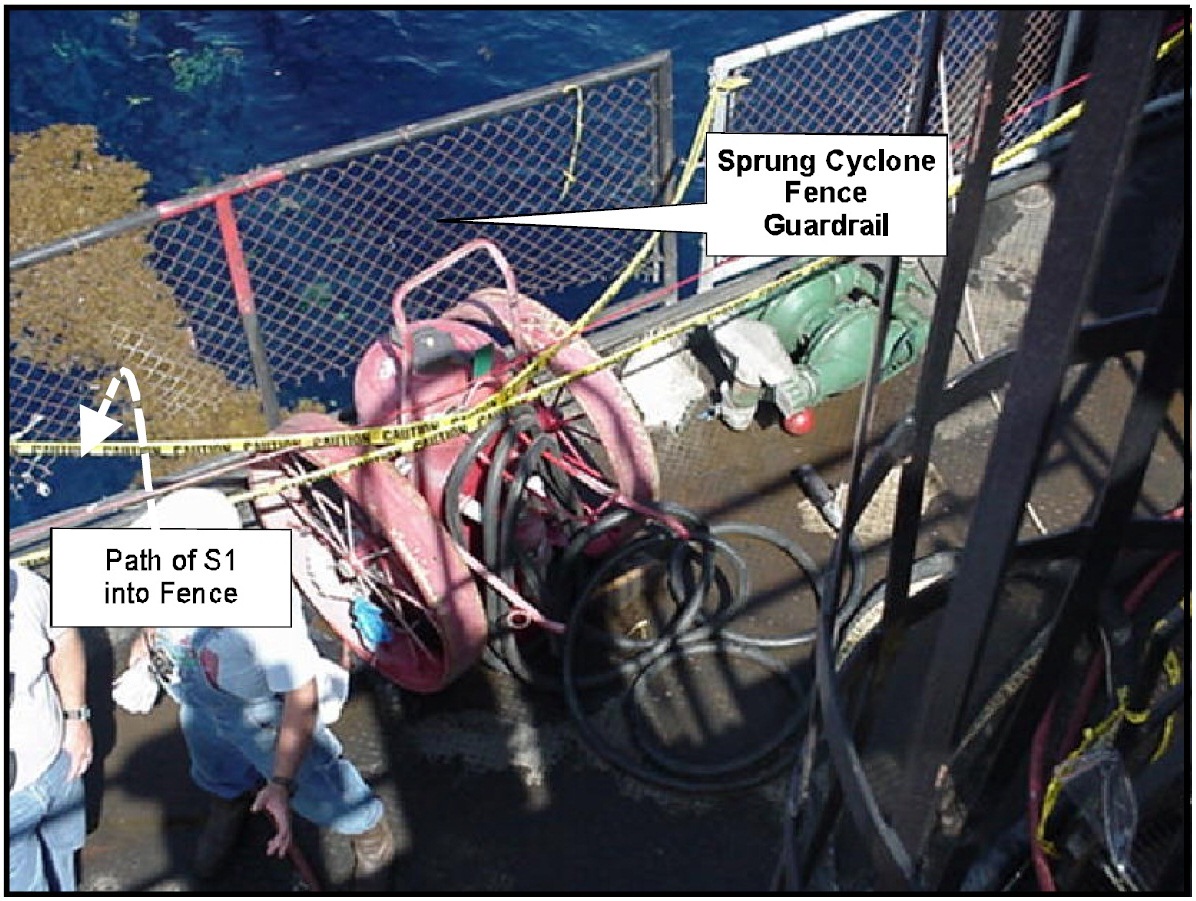
The same blast also directly impacted the summer employee who was standing next to the upper low-pressure separator foreman, about six feet from the open manway hatch of the lower low pressure separator. The summer employee was blown backward into the guardrail. (see photo below for picture of guardrail after explosion.) The guardrail in this area of the platformconsists of a regulation-height pipe frame with cyclone fencing attached to the frame with plasticties and/or cyclone material fasteners spaced about every four feet located around the rail and through the fencing. The bottom of the cyclone fencing in a 6- to 8-foot-long guardrail panel next to the one that was impacted was held in place by a single plastic wire tie. It is unknown how the guardrail fence panel impacted by the summer employee and foreman was secured to the frame. The guardrail frame the summer employee impacted was bent outward, and the cyclone fencing was sprung and deformed outward, leaving a significant gap at the bottom. Pieces of clothing were later discovered on the bottom of the fencing material (see photos below).

The impact of the blast then caused the summer employee to be thrown off of the platform into the water from a height of 50-70 feet, after first striking the guardrail. He sustained burns over
50-percent of his body from the fireball, the burns being mostly second degree with some first degree. He also sustained a broken rib and an injury to one of his legs.
The summer employee remained conscious after hitting the water but was entangled in something, possibly an air hose. In heavy seas he was able to disentangle himself and swim around the platform to the +10 landing from which a ladder was hung to within about six feet of the sea. By timing the waves, he was able to grasp the lower rung of the ladder and pull himself onto the plus-ten landing just as another crew member arrived to lend assistance.
On the main platform deck, the other members of the Contractor work crews administered to the injured. Two crew members had witnessed the summer employee being blown into the water. One ran to the rail and could see the summer employee swimming. As another crew member activated the man-overboard alarm, he ran down the stairs toward the +10 to see if he could help but did not access either a lifering or lifejackets from the storage bins to take with him. According to testimony, on the deck of the Platform there was considerable uncertainty about how many crew members were overboard because three hard hats were in the water. In the general confusion, no life rings were thrown to the man overboard.
After the summer employee pulled himself to safety, and was subsequently evacuated by stretcher up the stairs from the plus-ten deck, the injured crew members were all collected on the bridge of the Platform and emergency helicopter evacuation was called. The weather conditions were deteriorating and medivac helicopters were not immediately available. Therefore, after an elapse of about two hours, an Operator field helicopter landed and took the two worst injured, the summer employee and the foreman for the upper low-pressure separator, to a hospital onshore. Shortly thereafter, a medivac craft took the other two crew members, and a staff member who had been injured jumping out of bed at the sound of the alarm, to the same onshore hospital.
Root causes
During the accident investigation process the following have been identified as causes that led more or less to the accident
- No ventilation equipment was located near the lower low-pressure separator manway hatch, and the other entry point was unopened.
- A double block on the inlet line to the separator was noted, though the bleed valve, which some testimony indicated was not properly open and which may have been removed or replaced after the incident, may not have been operational.
- No skillets were found on the vent line, and the primary check valve was broken (although it was operational).
- The GASTECH model “Genesis” gas detection meter which was sent to SOLA Communications, Inc., for evaluation and readings test after the incident, found the meter to have corrosion on the inter connection board.
The explosive mixture in the separator originated from one of three possible sources:
- Gas transported from an outside source, into the vessel through existing piping connections, mixed with oxygen from the open manway.
- A flammable gas from some unknown source such as a non-hydrocarbon based mixture of soap spray.
- Gas generated from within the vessel mixed with oxygen from the open manway, including the possibility that the gas may have been present from the beginning of the cleaning operation.
The flash fire and blast was caused by a flammable mixture explosively igniting within the vessel. The flammable mixture was present in the vessel because of the following:
- The failure to initially vent the vessel according to policy and the failure to follow confined space entry procedures.
- The failure to vent the vessel continuously during entry.
- The failure to test the entire vessel properly for the presence of the flammable mixture prior to initiating confined space entry activities, which allowed the existence of the explosive conditions to be undetected.
Four separate violations of the Contractor policy involving confined space entry were noted in the period leading to the flash explosion, including requirements for initial and continuous ventilation, proper employment of gas detection in the entire area to be entered, donning proper protective gear and signing permits prior to breaking the plane of the hatch even to insert a gas detector.
In summary of all the above, the explosion was caused by the failure to open both hatches, ventilate, and continuously ventilate the vessel during entry, despite extensive pre-job procedural reviews. In addition, a gas detector was not deployed throughout the entire area of entry. These procedural failures occurred in part because of no managerial double-check of the actual operation. The injuries were caused by the explosion’s impact on personnel inside the vessel and immediately outside the open hatch. One man struck the guardrail cyclone fence material, springing it loose from its frame, before falling into the water. No flotation aids were thrown to him.
Lessons to be learned
- The operators should emphasize proper confined space entry procedure in the prejob safety meetings and have a second party confirm the procedures are being followed.
- Personnel not involved in a particular confined space entry should be made aware of the potential danger areas immediately outside any open hatchway of a vessel.
- Work crews should be reminded in safety meetings of the location of emergency flotation devices and the need to access them first in a man-overboard situation.
- Operators should review guard barrier ability to contain standard impacts, especially in the vicinity of major production equipment, vessels, and work areas.
Source: BSEE













Leave a Comment